3 Steps to Dosing Return to Run
Managing running workloads can be challenging. Ask any runner pushing their volume or intensity, this is a complex and deeply individual jigsaw puzzle. Adding in the element of injury recovery can make this process even more noisy. There are a number of factors to consider with a weaving web of interplay that will affect our return to run decision making, timeline, and the risk of re-injury upon return.
“Running experience and injury threshold seem to play a role in the relationship between training characteristics and development of injuries, while volume, duration, intensity, and frequency seem to have a complex interaction with each other which is not accounted for in the majority of the included studies”
- Nielsen et. al (2012)
With the inherent complexity of these modifiable and non-modifiable factors, we must simplify the problem to make sense of the issue and find a starting point for intervention. To do this, we can take a three step approach:
- Identify opportunity and risk based on the stage of injury recovery
- Categorize the issue to establish a trainable menu
- Define a starting dosage and anchor progression to subjective and objective tolerance measures
I. Identify Opportunity and Risk
Throughout the return to run process there will be varying levels of re-injury risk. It is our job to keep this risk as low as possible while preparing the individual to return to their prior level of function or beyond. Too much focal stress and we re-exacerbate the issue. Too little and we leave the runner vulnerable to re-injury upon return to normal training load. This is often a tricky balance to strike.
Nassim Taleb’s Barbell Strategy is a nice framework to help make sense of situations such as this and identify how to maximize opportunity while mitigating risk. Taleb’s barbell suggests that the bulk of investments should be made to either the general (low risk/low reward) “protect from the downside” buckets or the specific (high risk/high reward) “invest in the upside” buckets. Care should be taken to avoid the trap of the middle ground (moderate risk/moderate reward) (*cough cough slow jogging) between these.
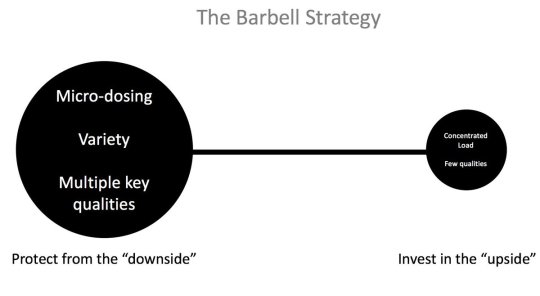
Credit: Jovanović M. Strength Training Manual: The Agile Periodization Approach.
In the return to run process, this model helps us to make sense of how to protect against downside while making calculated investments into specialized qualities that can pay dividends later on. For example, during a return to run recovery for a patellar tendinopathy, our primary focus must be in protecting from the downside (too much tendinous stress). During this time, the variety and our training methods should be relatively high and evenly distributed between general physical qualities (strength, endurance, ROM, elasticity,power etc..). This will help to maintain and improve base levels of fitness to “protect from the downside” of de-training. Concurrently, we can use a smaller amount of our resources on specificity. This can be a focus on specific qualities to “invest in the upside”. This may include stiff contact pogo hopping to increase foot ankle stiffness or low volumes of sprint work while we are still developing tolerance to normal running speeds and volumes. Early introduction of these more specific, higher intensity, qualities early on gives us a starting point to gauge tolerance while managing risk by slowly progressing dosage and choosing the stimulus wisely.
II. Categorization
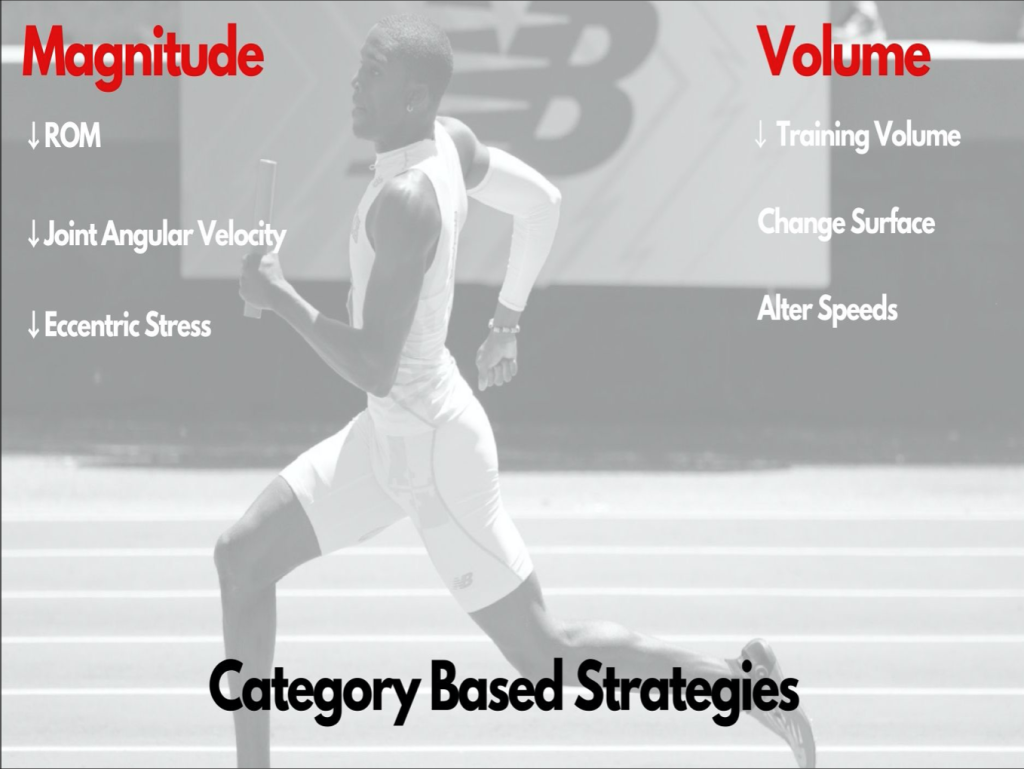
We can simplify injuries into either intensity/magnitude or volume related issues. These certainly have a degree of overlap, however, based on the likely primary driver of the injury, we can ascertain which stimuli need to be avoided to protect against the “downside” and where we can more safely begin to intervene.
Intensity/Magnitude
An example of a magnitude based injury would be a hamstring strain. The rate of force applied to the hamstring through a swing cycle created a tissue over-stretch and subsequent level of tearing of muscle fibers. Though there is likely an accumulation effect leading to the tissue vulnerability, for all intents and purposes the mechanism of injury is one of high force during one stride cycle. For a magnitude related issue, such as a strain, our primary concern is with the magnitude of force applied to the tissue. Specifically, the rate of loading of the hamstring as it lengths. Our manipulatable variables here will be centered around changing the range of motion of the activity and decreasing the angular velocity of the movement to decrease eccentric stress. We will need to be more cautious with the application of certain intensities but have more freedom to train at higher volumes.
An example of an upside investment opportunity in hamstring rehab is the accumulation of high volumes of sub maximal accelerations. Often, we are able to accumulate as much as 3 sets of 10, 10 meter accelerations. This is a high volume of work that will help to maintain sprint patterning and general tissue preparedness without stressing the vulnerable tissue since the rate of loading of a hamstring is quite low in the first 10 meters of acceleration. This leads us into a window of opportunity for a more volume based entry point for return to run.
Volume
For a volume related issue such as shin splints, while the intensity is certainly a consideration, our main determinants of tolerance will likely be more volume based. Within this categorization our primary controls will be modulating training volume, and changing the surface and speeds to manipulate impact forces. In the initial stages for example, the runner may be able to tolerate high intensity jumping or sprinting at low volumes. This leaves us with a more intensity biased program as an entry point into return to running.
III. How to Dose?
These categorizations can simply provide a suggested starting point. I find this useful but it is certainly imperfect. The power in this process is the permission to train harder, earlier, and more safely through finding the tolerable opportunities. Ultimately, any intervention delivered must be gradually increased in volume and intensity and anchored to subjective and objective measurements of tolerance for the individual runner. Simply put, we must pick a starting dosage and slowly titrate this while gauging tolerance.
Sets and Reps
There is no magic recipe for the number of sets, reps, or total distance the runner should be able to tolerate at any given stage. The best method is to simply start with a very conservative dose and titrate from there. I will typically make a best guess at what volume I expect the runner to be able to tolerate based on their previous training volumes, current level of impairment, and subjective pain experience. I then decrease this by ~10% and start there. Once we find a tolerable baseline level we can slowly titrate up from there typically with session to session changes no greater than 10-20%.
Anchors
Subjective pain experience in most circumstances is the best measure to glean tolerance. Setting a max acceptable pain threshold for the runner (i.e no greater than 3/10) is a good way to monitor this and give the runner ownership over the daily training decision making. Another avenue to track tolerance for certain issues is repeated range of motion measures. For instance, in hamstring strain rehab, the use of a Max Hip Flexion Active Knee Extension (MHFAKE) assessment can be a decent indicator of how volumes and intensities are being tolerated. Throughout the recovery process, you should see an increase in the range of motion. If at any time you see a regression, this may be a sign that the hamstring is protectively “tightening” due to intolerance of dosage. For an ankle or lower leg injury, weight bearing ankle dorsiflexion (posterior tissue injury) or plantaflexion (anterior tissue injury) may be a good repeat test.
Wrapping up
Return to run is an imperfect process. A pre-fabricated plan with pre-set progression is far inferior to agile planning with room to adjust. By categorizing the issue, identifying risks and opportunities, and anchoring dosage to indicators, we can maximize opportunities while having guardrails to keep us from driving off of the road.
– Dr. Anthony Iannarino, Site Director – Rehab 2 Perform™, Bethesda
References:
- Nielsen RO, Bertelsen ML, Møller M, et al. Training load and structure-specific load: applications for sport injury causality and data analyses. Br J Sports Med. 2018;52(16):1016-1017.
- Taleb NN. Antifragile: Things That Gain from Disorder. 1st edition. Penguin; 2012.
- Credit: Jovanović M. Strength Training Manual: The Agile Periodization Approach.
FUEL UP
Listen: Clinical Athlete Podcast Episode 89: Return to Sprinting with Dan Lorenz
- Return to sprint can often be an intimidating process to guide a client through. When do we start? Are we dosing appropriately? Dan Lorenz does an excellent job elucidating key objective measures to guide the return to sprint process rather than simply following timelines or blind prescriptions.
Educate: Differential Effects of Fatigue on Movement Variability
- Movement variability can certainly be a confusing concept to understand even without the added element of fatigue. Cortes et al do an excellent job of “wading in the gray” on this topic while providing useful clinical context. Give it a read!
- Cortes N, Onate J, Morrison S. Differential effects of fatigue on movement variability. Gait Posture. 2014;39(3):888-893.
Read: The Brain That Changes Itself: Stories of Personal Triumph from the Frontiers of Brain Science by Norman Doidge, MD
- Neuroplasticity is a fascinating topic. Doidge delves into some of the discoveries and continued questions in the evolving field through this entertaining book.
Engage: @ignitephyzio
- Ziad and the team over at Ignite Phyzio in Orange County California do an excellent job “showing their math” in their return to sport process. By demonstrating practical solutions to strength testing and novel strategies for return to sport preparation, their IG has become a useful resource for clinicians and coaches.